
Back in the day, late 1930’s, a psychiatrists by the name of Ugo Cerletti and Lucio Bini performed the first electroconvulsive therapy (ECT). Surprisingly, this was not the worst treatment doctors experimented with on patients suffering from schizophrenia. Doctors also used Insulin coma therapy, this began around 1933 and ended in the 1950s. Some patients died as doctors attempted to bring them out of the insulin induced comas.
Ladislas Meduna would induce seizures in patients by injecting them with camphor. He hypothesized that there was a biological antagonism between schizophrenia and epilepsy. The seizures would lead to reduced schizophrenic symptoms. His methods were used until ECT was established. Pharmacological treatments would come in waves, they’d use meds for a couple years and, like a fad, interest would fade. It wasn’t until the 1980’s that pharmacological treatments finally gained a strong foothold and have since remained the leading method by which doctors treat psychological illnesses.
What’s interesting is that ECT never truly faded into the history books with the likes of lobotomies or insulin coma therapy. ECT stuck around and is currently used to treat patients with Major Depressive Disorder, Mania, and Schizophrenia. Which is really weird because it sounds like such an archaic and barbaric treatment when juxtaposed with pharmaceuticals. Granted, pharmaceuticals are not perfect. They come with many side effects and some of them can be lethal if not taken appropriately. Especially when it comes to medications that will interfere with our brain chemistry.

Take lithium, a mood-stabilizing agent, used to treat bipolar disorders and mania. Works really well but has some nasty side effects if serum concentrations go above 1.5 mEq/L like seizures, ataxia, circulatory failure, coma, and death. But patients, on average, respond well to it. For those that don’t respond well to medications like lithium, benzodiazepines, antipsychotics, and MAOIs, they are left with one alternative, ECT.
ECT is quite the controversial treatment even in the medical field. Some people believe that the benefits come at the cost of brain damage. Some studies have shown that brain damage is not what is occurring. The details of how ECT causes a therapeutic response is unknown, however, what is known is that seizures do change the chemistry in our brain and those changes compound on one another. Affected neurotransmitters include serotonin, norepinephrine, and dopamine, the same biogenic amines that are affected by antidepressant drugs.
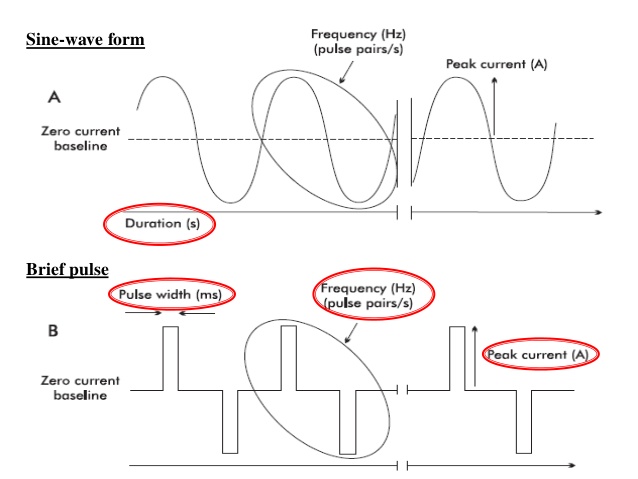
Like all other treatments, ECT comes with some side effects. The most commonly seen are short term memory loss and confusion. Most patients return to their cognitive baseline around 6 months. For those that report prolonged memory impairment also tend to show little improvement with ECT. Stimulation by sine wave (continuous) current resulted in greater memory impairment, both long and short term, than when compared to short-pulse wave (intermittent) current.

It’s not only an interesting procedure to perform and observe but the data seems to back up the beneficial claims of ECT therapy. The procedure itself is not all that violent. Patients are put under using an anesthetic, like Propofol. They are then given a muscle relaxer to limit or prevent any muscular spams and caffeine citrate IV to decrease the seizure threshold, plus whatever the anesthesiologist deems appropriate.

The procedure, from entry to the procedure room to arrival at the post surgical area, took approximately 20 minutes. You do see some jaw clenching but thats expected considering the location of the electrodes. It’s very anticlimactic, which bodes well for the patient. I wonder if ECT will ever go mainstream or is the stigma of “electro shock therapy” too great a stain to overcome.
References
Psychiatric Mental health concepts of care in evidence-based practice
